Medical Sales Director | Community Health Educator | Wellness Innovator
Last updated on abril 24, 2026
The state of Texas has set a national gold standard for Remote Patient Monitoring (RPM) and telemonitoring services. Through progressive legislation like House Bill 2727 and a collaborative care model uniting prescribing physicians with 24/7 Home Health Agencies (HHAs), Texas Medicaid has dramatically improved health outcomes for high – risk residents. House Bill 2727 officially clarified that the term “home telemonitoring service” is synonymous with “remote patient monitoring” (RPM). By reducing the clinical barrier to entry – now requiring only one risk factor for diabetic and hypertensive patients—Texas has successfully expanded access to life-saving technology.
With the introduction of the new 2026 RPM billing codes and guidelines, the Lone Star State is empowering medical practices to deliver precision, data-driven care while optimizing their revenue cycle. The AMA expanded the RPM code set to include new time-based options for shorter monitoring periods and lighter management, which closes previous billing gaps.1 Whether you are a local patient seeking proactive health management or a clinical provider aiming for seamless compliance, understanding the Texas Medicaid RPM framework is crucial.
Below is an authoritative guide formatted for patients, physicians, and home health agencies navigating the Texas digital health landscape in 2026.
5 Questions a Texas Resident Should Ask to See if They Are a Candidate for RPM
If you are a Texas resident exploring Medicaid-funded remote patient monitoring under 2026 guidance, ask your doctor these five questions:
Do I meet the clinical condition criteria? Ask if your diagnosis of diabetes, hypertension, or both qualifies you for the program. (Note: Patients 20 years and younger with end-stage solid organ disease, transplants, or mechanical ventilation needs also qualify).
Do I have at least one qualifying risk factor? Ask if your medical history includes at least one Texas-mandated risk factor, such as two or more hospitalizations in the last 12 months, frequent ER visits, poor medication adherence, documented risk of falls, or care access challenges.
Will I receive an FDA-cleared device for automatic tracking? Ask if the partnering Home Health Agency will provide you with a connected, FDA-cleared device (like a blood pressure monitor or glucometer) that automatically transmits data, eliminating the need for you to manually log numbers.
Does my care plan align with 2026 transmission guidelines? Ask if you are expected to transmit data for standard continuous monitoring (16 or more days a month) or if you qualify for short-term monitoring scenarios (2 to 15 days a month) recognized under the new 2026 guidelines.
Will my health data be monitored around the clock? Ask if the Home Health Agency providing your device maintains 24/7 availability to track your vitals and immediately notify your physician if your readings become dangerous. Additionally, patients should be aware that their health data must be automatically transmitted by the device, as self-reported data is not sufficient for RPM billing.
5 Questions Physicians Need to Ask Before Enrolling Patients
For Texas physicians, teaming up with a Home Health Agency to provide RPM is highly beneficial, but requires strict compliance. Ask yourself these five questions:
Have I established and approved a highly specific Plan of Care? Does the patient have a formally documented Plan of Care featuring individualized outcome measures that I have reviewed and shared with the partnering Home Health Agency?
Does my patient meet the updated HB 2727 risk-factor threshold? Have I clearly documented in the EHR the single qualifying risk factor (e.g., fall risk or frequent ER visits) required by Texas Medicaid to justify medical necessity for diabetic or hypertensive patients?
Is my billing department prepared for the 2026 CPT code updates? Are we ready to utilize the new 2026 codes, such as billing CPT 99445 for shorter 2-15 day monitoring periods, or CPT 99470 for the first 10 to 19 minutes of clinical treatment management?
Is the partnering Home Health Agency fully compliant with Texas regulations? Is the HHA capable of handling the physical device logistics, patient education, and providing the legally mandated 24-hour, 7-day-a-week data monitoring and triage?
Are we tracking fractional minutes to prevent OIG audit risks? Does our IT platform natively track the exact minutes of interactive clinical communication and data transmission days to ensure we meet stringent state and federal compliance audits? Physicians must also ensure they have an established relationship with the patient, including a prior in-person or telehealth visit, before initiating Medicare RPM services.3
10 FAQs: Do's and Don'ts for Providing and Receiving RPM Services in Texas
What is the correct Texas Medicaid billing code for home telemonitoring?
Do: Ensure Home Health Agencies and hospitals bill using procedure code S9110 accompanied by revenue code 780. You must also append the correct U-modifier (U2 through U9) corresponding to the exact number of transmission days achieved within a rolling month.
Can patients self-report their daily health data?
Don’t: Rely on patients to manually write down or self-report their physiological data.
Do: Ensure data is electronically collected and automatically uploaded by an FDA-defined medical device to a secure, HIPAA-compliant location.
Do telemonitoring services require prior authorization in Texas?
Do: Obtain prior authorization before starting services. Under Texas Medicaid, procedure code S9110 requires prior authorization, which can be approved for up to 180 days.
How do we bill the new 2026 short-term device supply codes?
Don’t: Bill the new CPT code 99445 (2-15 days of data) concurrently with CPT 99454 (16-30 days of data) for the same patient.
Do: Choose the single most appropriate code based on the exact number of days the patient transmitted data in that 30-day period.
What is the protocol for abnormal patient readings?
Do: HHAs must have a registered nurse (RN), clinical nurse specialist (CNS), or physician assistant (PA) actively review the data. If a reading falls outside the parameters set by the physician’s Plan of Care, the HHA must immediately report it to the prescribing physician.
Can we bill the new 2026 10-minute management code with the 20-minute code?
Don’t: Bill the new CPT 99470 (first 10 minutes of management) and CPT 99457 (first 20 minutes) together.
Do: Use 99470 only when management time is strictly between 10 and 19 minutes. If interactive time reaches 20 minutes or more, bill 99457 instead.
Is patient consent required before deploying devices?
Do: Obtain and clearly document informed patient consent in the medical record prior to initiating any RPM services or billing CMS/Medicaid codes.
Do HHAs need to report to the physician if the patient’s vitals are perfectly normal?
Do: Yes. Even in the absence of anomalous readings, scheduled periodic reporting of the patient’s data to the prescribing physician is legally required at least once per calendar month.
How is the initial device setup billed?
Do: The HHA should bill for the initial setup and patient education using S9110 with modifier U1. This is generally reimbursed one time per episode of care, unless documented extenuating circumstances require a new setup.
How do Federally Qualified Health Centers (FQHCs) and Rural Health Clinics (RHCs) bill for this?
Don’t: FQHCs and RHCs should not use the retired bundled code G0511, as the CMS transition period has ended and the code is now officially terminated for these services.
Do: FQHCs and RHCs must now bill for care management and remote patient monitoring using the individual CPT codes (e.g., 99453, 99454, 99445, 99457, 99470, 99458) just like non-rural providers, reflecting the exact data transmission days and treatment management time provided. Furthermore, the OIG has highlighted the importance of avoiding billing for a high proportion of enrollees who have no prior history with the medical practice to reduce program integrity risks.
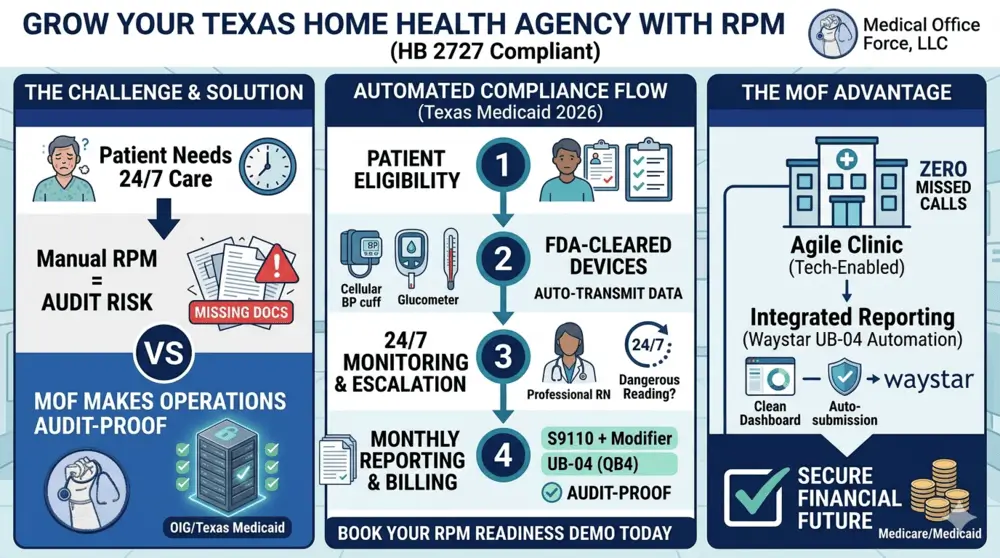
The End-to-End Texas Medicaid RPM Process: Ensuring OIG and Audit Compliance
To successfully implement a Remote Patient Monitoring program that is fully compliant with Texas Medicaid and thoroughly protected against Office of Inspector General (OIG) audits, physicians and Home Health Agencies must follow a strict, well-documented operational sequence. Relying on a well-developed Electronic Medical Record (EMR) or specialized RPM software platform to automatically capture data at every point is the most effective way to make the service fully OIG and Medicaid audit-proof.
Patient Selection: The process begins with identifying eligible Medicaid clients diagnosed with conditions like diabetes or hypertension who exhibit at least one state-mandated risk factor (e.g., frequent ER visits, risk of falls, or poor medication adherence).
Physician Order and Care Plan: The prescribing physician formally issues an order for home telemonitoring. Based on this order, the HHA establishes a patient-specific Plan of Care detailing individualized outcome measures and safe vital sign parameters. Crucially, the physician must review and approve this precise Plan of Care.
Delivery of Cellular Devices: The HHA provides the patient with FDA-cleared, cellular-connected medical devices (such as blood pressure cuffs or glucometers) directly to their home. The HHA is responsible for the initial equipment setup and patient education regarding device usage.
Daily Vital Sign Collection: The patient uses the device daily to collect their physiological data. Because the devices are cellular-enabled, this data is automatically and securely transmitted to the HHA’s HIPAA-compliant software platform, completely bypassing the risks of patient self-reporting.
24/7/365 Monitoring and Escalation: Texas Medicaid mandates that telemonitoring providers remain available 24 hours a day, 7 days a week. Clinical staff at the HHA continuously monitor the incoming data. If a patient’s vital signs fall outside the safe parameters established in the physician’s Plan of Care, the HHA immediately responds and escalates the alert to the prescribing physician for rapid medical intervention.
6. Monthly Reporting and Audit-Proof Billing: Even if no anomalous readings occur, the HHA must generate a scheduled periodic report of the patient’s data for the physician at least once per calendar month. At the end of the 30-day monitoring period, the EMR system aggregates the exact number of transmission days and interactive clinical minutes. This comprehensive monthly report captures all events and time logs, allowing the HHA to accurately bill Medicaid (using procedure code S9110 and appropriate U-modifiers) and the physician to safely bill the corresponding CPT codes. By utilizing an advanced EMR platform to automatically track and timestamp these mandatory components, providers eliminate manual errors and ensure their billing stands up to rigorous OIG scrutiny. Recent OIG reports indicate that missing treatment management documentation is a leading cause of audit failures, emphasizing the need for comprehensive EMR tracking.5
Process Automation: Managing UB-04 (QB4) Claims via Waystar
While standard procedure codes like S9110 are utilized by many providers, institutional billing often requires the UB-04 form (also known as the CMS-1450), which is the standard institutional claim form used by hospitals and facilities to bill insurance payers. The term “QB4” is frequently used as a phonetic or shorthand reference to the UB-04.
Within the Waystar revenue cycle platform, this form is processed primarily through automated electronic workflows rather than manual paper entry, ensuring speed and accuracy. Automated billing platforms are crucial since Medicaid payments for clinical services must strictly adhere to state and federal fee schedules.6
How the UB-04 (QB4) Gets Input into Waystar
Waystar typically receives data for these forms through three main methods:
PMS/EHR Integration: Most data is automatically pulled from a provider’s Practice Management System (PMS) or Electronic Health Record (EHR) like Epic. When a claim is “sent” from the clinical side, it maps directly into Waystar’s electronic 837I format (the digital version of the UB-04).
SFTP & EDI Uploads: High volumes of claims are often uploaded via Secure FTP (SFTP) using standardized EDI connection settings.
Manual Entry (Correction): If a claim has an error, users can “open” the claim within the Waystar Portal to manually edit specific fields (Form Locators) before resubmission.
Example of UB-04 (QB4) Data Fields
The form is organized into “Form Locators” (FL). Below are common fields you would see in a Waystar claim editor:
Form Locator (FL)
Field Name
Description Example
FL 01
Billing Provider
Hospital Name, Address, and NPI
FL 04
Type of Bill
A 4-digit code (e.g., 0111 for Inpatient Admit through Discharge)
FL 12–15
Admission Info
Date, hour, priority, and source of admission
FL 17
Patient Status
Code indicating where the patient went (e.g., 01 for "Discharged to Home")
FL 42
Revenue Codes
4-digit codes for specific departments (e.g., 0250 for Pharmacy)
FL 67
Principal Diagnosis
The primary ICD-10 code for the visit
Automated Enhancements
Waystar uses AI-powered tools to “scrub” these forms as they come in:
Claim Edits: The system automatically checks for missing NPIs or invalid ICD-10 codes.
Attachment Automation: If the claim requires supporting clinical notes, Waystar can automatically attach PDF or TIFF files to the electronic submission.
References
Texas Legislature, House Bill 2727 (88th Legislature).



Insightful overview of Texas RPM updates.