Medical Director, Medical Office Force LLC | Athens, Georgia
Alumnus: SMS Medical College, Emory University, University of Alabama at Birmingham
Last updated on abril 13, 2026
Summary
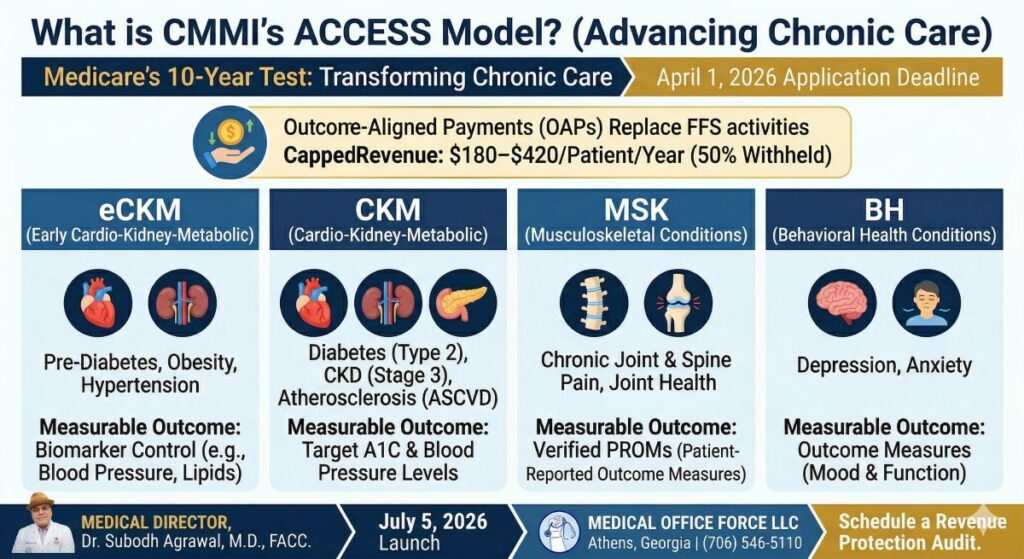
The ACCESS Model is a 10-year voluntary Medicare initiative designed to scale chronic care management through technology and Outcome-Aligned Payments (OAP). According to the official CMS ACCESS Model overview, it focuses on four clinical tracks and ties 50% of reimbursement to measurable clinical improvements.
The CMS Innovation Center (CMMI) introduced the Advancing Chronic Care with Effective, Scalable Solutions (ACCESS) Model to transform how Medicare beneficiaries with chronic conditions receive care. This model moves away from Fee-For-Service (FFS) toward a “scalable,” digital-first approach.
The 4 Clinical Tracks of the ACCESS Model
The model is structured around four distinct tracks. Practices can participate in one or more, depending on their specialty:
Early Cardio-Kidney-Metabolic (eCKM): Focuses on hypertension, obesity, and pre-diabetes management.
Cardio-Kidney-Metabolic (CKM): Designed for patients with established heart disease, CKD (Stage 3), and Type 2 diabetes.
Musculoskeletal (MSK): Targets chronic pain and joint health management.
Behavioral Health (BH): Focuses on depression, anxiety, and integrated mental health care.
The Payment Logic: How Do OAPs Work?
The ACCESS model utilizes Outcome-Aligned Payments (OAPs) instead of traditional care management codes (like CCM or RPM). As detailed in the CMS Financial Structure and Clinical Performance guide, the payments are two-tiered:
Year 1 (Initial Year): A higher payment range ($180 – $420 per patient) to cover technology onboarding.
Follow-on Years: A lower maintenance payment range ($90 – $210 per patient).
The 50% Clinical Outcome Adjustment: CMS withholds half of the payment, only releasing it if specific benchmarks (like blood pressure or A1C control) are met.
Key Deadlines for 2026
April 1, 2026: Application deadline for the first cohort.
July 5, 2026: Official launch of the first performance year.
2033: Expected conclusion of the 10-year test period.
Frequently Asked Questions (FAQ)
How does ACCESS coordinate with my Primary Care Provider?
The model is designed to complement traditional care. Referring clinicians can receive electronic updates on patient progress and may bill a new co-management payment for reviewing these updates and coordinating care.
What are the technical requirements for participants?
Organizations must use secure, interoperable systems, including CMS APIs for enrollment and reporting. They must also designate a physician Clinical Director to oversee quality and compliance. Learn more about IT Infrastructure Support here.
What is the “FFS Exclusion Policy”?
CMS prevents “double-dipping.” If a patient is aligned with an ACCESS participant for a specific condition, other providers cannot bill overlapping services like Chronic Care Management (CCM) or Remote Patient Monitoring (RPM) for that same condition.
Strategic Verdict
The ACCESS model offers massive scale but creates a significant revenue gap for traditional clinics. Before transitioning, you must analyze your billing data.



For more information, write to contact@medicalofficeforce.com
Share Your Thoughts
No comments yet — be the first to comment!