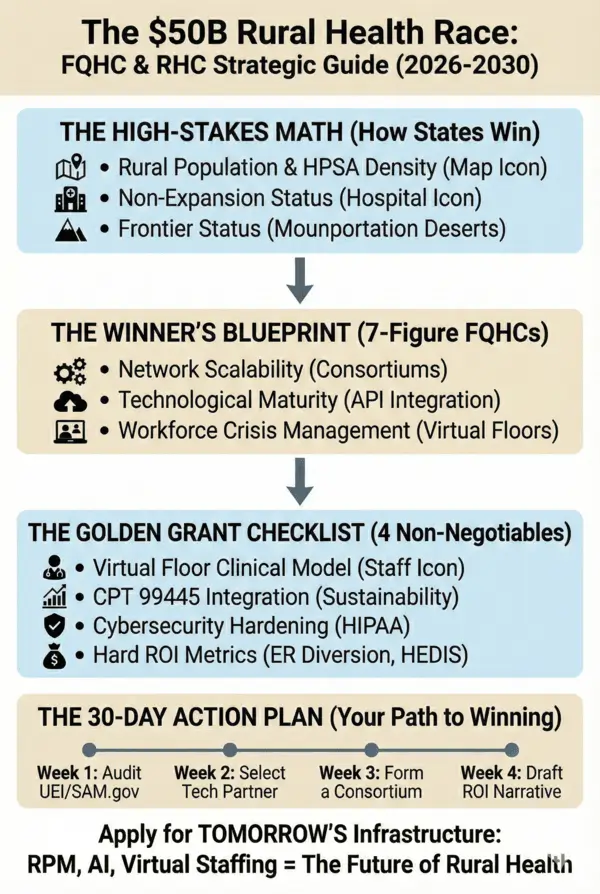
Successful proposals increasingly include four non-negotiable components.
A. Virtual Clinical Infrastructure
Funding requests focused solely on local hiring are frequently denied. Instead, reviewers expect hybrid staffing models that blend onsite care with remote clinical capacity.
The underlying logic is simple: funding must translate into access, not vacancies.
Language that consistently resonates includes:
“Ensuring clinical continuity through augmented remote staffing.”
B. Revenue Sustainability Through RPM and Digital Care
Grant programs are no longer designed as long-term operating subsidies. They are bridge investments.
Explicit integration of CMS RPM and digital care pathways particularly the 2026 CPT 99445 structures, signals that services will remain financially viable after grant periods conclude.
Key positioning:
“Financial sustainability through CMS-aligned remote care reimbursement models.”
C. Cybersecurity and Compliance Readiness
A growing portion of rural funding is earmarked for digital security. Data breaches in under-resourced systems now represent systemic risk, not isolated events.
Strong proposals address:
- SOC2-aligned controls
- Encrypted patient-device communication
- HIPAA-compliant cloud architecture
This is no longer optional infrastructure. It is foundational.
D. Outcome-Based ROI Commitments
States must justify these investments to legislatures and federal auditors. Soft narratives are insufficient.
Competitive applications quantify:
- 20–25% reduction in non-emergent ER utilization
- 10–15% improvement in HEDIS/MIPS quality metrics
- Measurable reduction in per-member-per-month Medicaid spend
The underlying question is always: “What will this save the system?”


Great to know and growth to go
Informative.
Informative!
Great Information
Appreciate the insights shared—very informative and valuable
This is a sharp, timely reality check. By reframing rural funding as a performance driven investment in execution capacity rather than a needs-based grant, you highlight what many clinics still miss. A must read for FQHCs and RHCs that want to compete, not just comply in the 2026-2030 cycle!!
Appreciate the insights shared—very informative and valuable
Very informative as this will help healthcare to improve in rural areas.
Great information
Fantastic
Great reminder that the right priorities can make a big difference in healthcare.
The $50B rural health race is real—and clinics that invest early in technology, strong revenue cycle management, and patient access will win. Those that delay adapting risk falling behind as funding, payers, and patients shift toward value, efficiency, and outcomes.
Quite Informative! Thanks.
This blog accurately reflects how funding decisions are shifting from need alone to execution and measurable outcomes. Well done, please keep posting insights like this.
VERY INFORMATIVE , AND CONSIDERATE !
Sharp, timely, and grounded in how CMS actually thinks. It clearly shows this isn’t grant chasing, it’s a survival and scale strategy for rural clinics
Highly informative with excellent insights
Great Information .
Great information !!
Good insight into where rural health funding is really headed.
Essential reading for anyone tracking rural health funding trends
Sharp, timely, and grounded in how CMS actually thinks. It clearly shows this isn’t grant chasing, it’s a survival and scale strategy for rural clinics
Very useful information with great Insights.
Great work! clinics that align with these priorities will not only secure funding as well as they will stabilize margins, improve workforce resilience, and expand access in markets that have historically struggled to survive.
Very Informative!
This is great for the healthcare and win win situation for patients ,Great information shared.
Great information !!
Concise and informative overview of the evolving rural health funding priorities……
Great Information!
Good insight into where rural health funding is really headed.
Looking forward to learning more about the $50 Billion Rural Health Race Plan and the strategy to accelerate growth in rural health
Very informative for the health and wealth.
Looking forward to learning more about the $50 Billion Rural Health Race Plan and the strategy to accelerate growth in rural health.
Great information !!
excellent information
I loved to know that clinics that align with these priorities will not only secure funding but also stabilize margins, improve workforce resilience, and expand access in healthcare.
Informative
Great insights on how rural clinics can leverage the $50B health transformation funds.