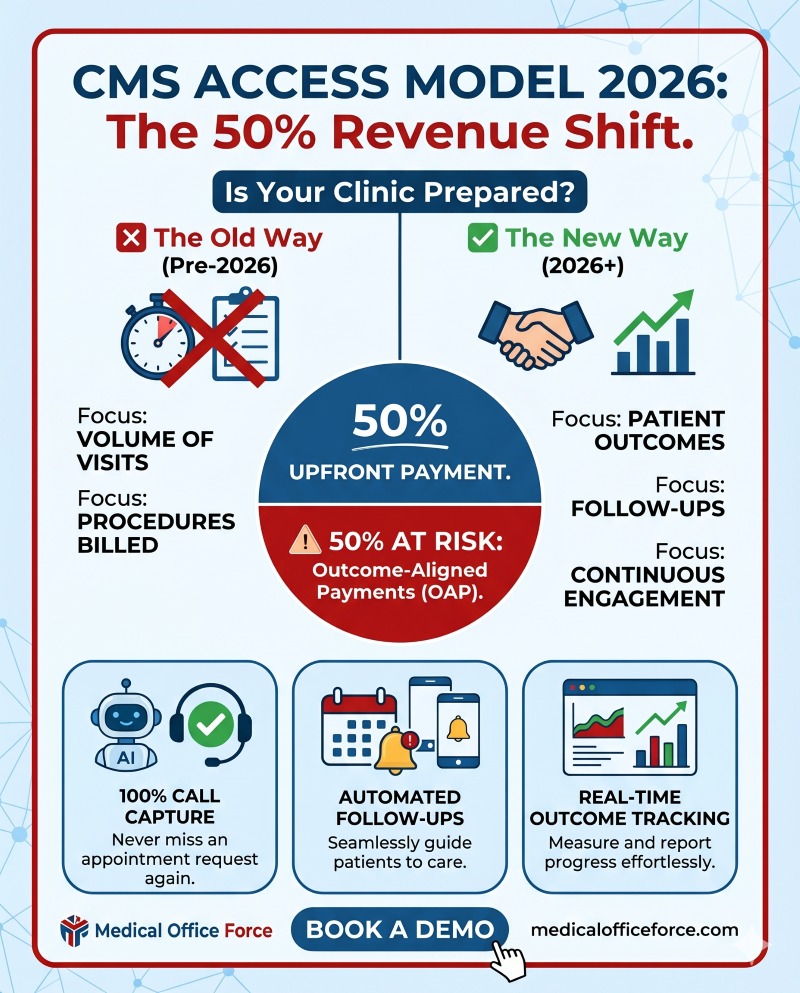
The CMS ACCESS Model rewards agility. Small clinics that leverage technology can respond faster, build deeper patient relationships, and maintain higher engagement rates than bloated hospital systems.
Conclusion: Adapt or Fall Behind
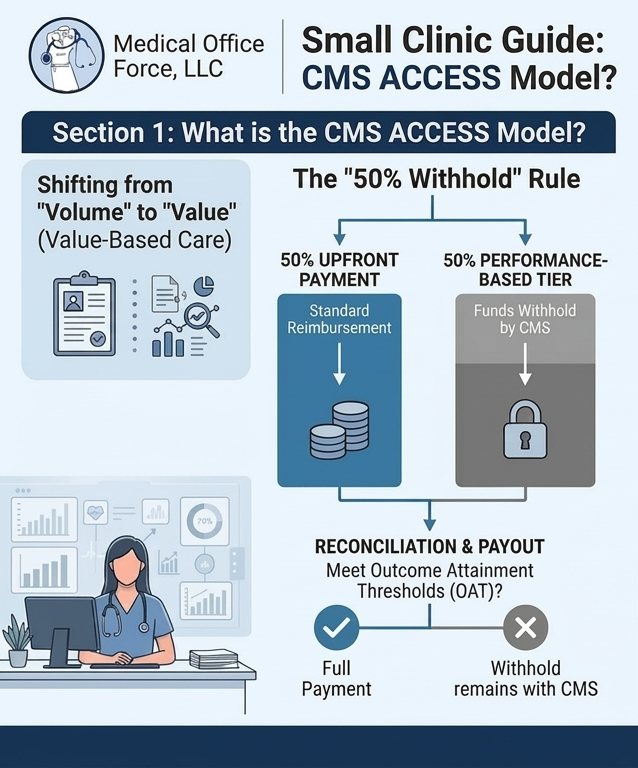
The CMS ACCESS Model is a fundamental shift in healthcare economics. By investing in patient engagement and AI-driven automation today, your clinic can secure its financial future and outperform the competition.